
The burden of urinary tract infections: challenges and solutions

With urinary tract infections being both a burden on the health system and a contributor to antimicrobial resistance, Jonathan Shaw says that advanced diagnostics can play a key role.
Urinary tract infections (UTIs) constitute some of the most common bacterial infections treated in the UK. While often perceived as minor and transient, UTIs pose a significant challenge to public health, with rising levels of antimicrobial resistance (AMR) adding further complexity to an already demanding clinical landscape. The burden of UTIs is felt at every level of the UK's healthcare system, from general practice to clinical laboratories.
This begs the question, what can be done to help improve the situation? The dominance of UTIs as a clinical target will likely persist, and in a clinical landscape looking to strengthen its antibiotic stewardship, solutions that are cost-effective, accurate and that have a quick turnaround time (TAT) need to be widely available.
This short blog will investigate this burden, focusing on: the statistics surrounding UTI analysis; the challenges that our health system faces; and the solutions that could be used to help lessen the burden and improve patient outcomes.
Challenges
Urinary tract infections are noted as the most common bacterial infections overall both for men and women in all patient care settings, while disproportionately affecting women and older adults.1 Patients presenting with UTIs account for a signification proportion of primary care appointments, and consequently, urinalysis testing in clinical laboratories presents a considerable time and resource sink.2
As a result of such a high prevalence, it is no surprise that there is a remarkably high use of antibiotics against UTIs. In England, at a primary care level, 18% of all antibiotics prescribed were to treat lower or recurrent UTIs.3 A study of 587 general practices showed that between 2000 and 2015, prescriptions of antibiotics for UTIs were the third most numerous, only behind prescriptions for upper and lower respiratory tract infections.4 It also presented that UTIs had the highest prescription rate, coming in at 89.4%. Such a high prescription rate indicates UTI treatment should be one of the key targets for confronting the issue of AMR.
At a primary care level, it can be safely assumed that, in most cases, antibiotic prescriptions are provided in line with correct operating procedures and that resulting treatments are, therefore, applied correctly. Primary care is often limited by the point-of-care tests (POCT) available, yet they provide a fantastic service with the tools they have at their disposal.
However, current UTI POCT involves using dipstick tests that, while being a quick and accessible test, are not always accurate. The test strips identify leucocyte esterase, nitrite levels and blood, which provide little to no information on the pathogenic cause of the infection.5 It is important to note that no two UTIs are the same, with each infection containing different pathogens with different resistance profiles. Using a non-specific test may lead to the over prescription of broad-spectrum antibiotics in cases where a mor patient-targeted approach was required. As levels of resistance to broad-spectrum antibiotics rise, they will become less effective, increasing the likelihood of patients presenting back to primary care following unsuccessful treatment. There are also instances where patients with recurring symptoms, who also produce negative dipstick test results, may also be prescribed non-specific antibiotics - potentially unnecessarily - theoretically contributing to the growing burden of AMR.
At a secondary/tertiary care level, the latest data (2022-2023) presented that 18% of the 1.9 million emergency admission for bacterial infection and/or sepsis in England (~335,000 cases) had a UTI clinical code attributed to the patient during their admission.3
Additionally, latest statistic (2018-2023) estimated that UTI infections as a primary diagnosis accounted for 800,000 hospital admissions.6 Data also show that, in this same period, over 50% of the 800,00 hospital admissions were related to patients aged 70 and over, with an average hospital stay of 17 days.3 (See fig 1.) UTIs are also the second biggest contributor to hospital-acquired infections (HAI).7 The vulnerability of the admittees (as a result of their age), in addition to the likelihood of comorbidities, heightens the risk of patients contracting HAI-UTI, highlighting the need for clinical laboratories to have access to technology that provides accurate results promptly.
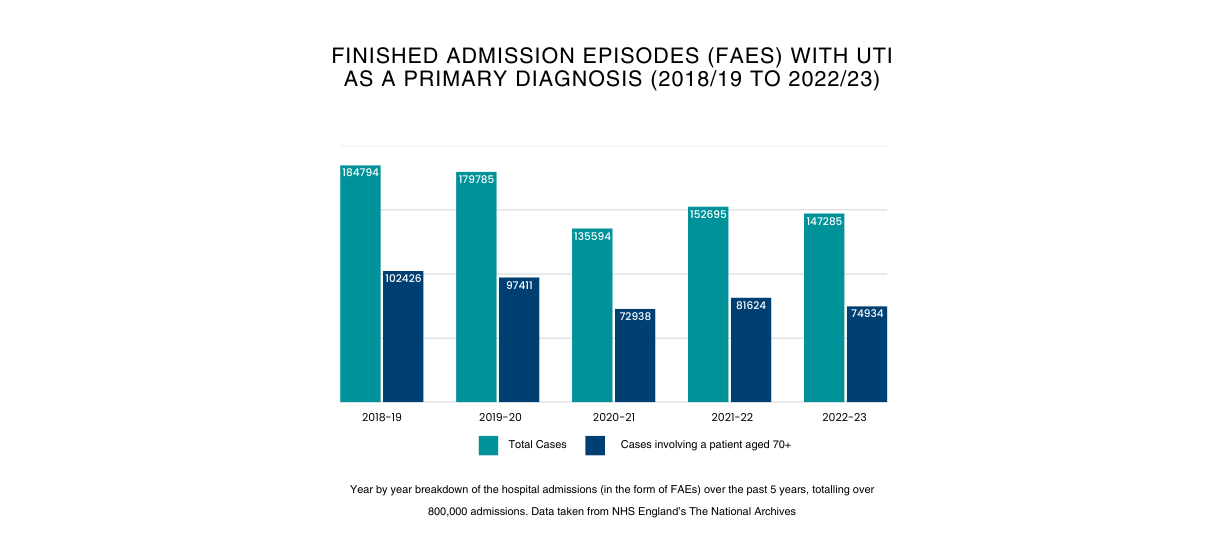
Figure 1
Rising levels of AMR in urinary pathogens is also a growing concern. Approximately 25% of urine samples in the first half of 2023 contained bacteria resistant to a common antibiotic.8 In 2023, there were 66,730 recorded serious antibiotic-resistant infections in the UK, a rise of over 4,400 infections (7%) compared to 20196, with 65% of bloodstream infections involving Escherichia coli,6 the most common causative pathogen of UTIs.
A combination of the rising hospital admission numbers and the increasing resistance profile of E. coli urosepsis (as a result of bacteraemia) continues to intensify as a serious issue. Urosepsis was the topic of a previous Pathology in Practice article back in 2014 (which also discussed Mast Group's previous urinalysis solution, the Mast Uri System). This article highlighted the blue of retrieving antibiotic sensitivity results promptly to aid in prescribing narrow-spectrum antibiotics, decreasing the use of unnecessary antibiotics,9 and shows that despite a decade of innovation, the risk of urosepsis remains a real threat.,
Solutions
Published in July 2025, the '10 Year Health Plan for England: fit for the future' stated that science and technology is being realigned as a primary focus for the NHS. The plan remarked on how the NHS is currently "behind the technological curve" and that prioritising it will be key to bringing " cutting-edge care to all patients". 10 This ambitious plan discussed advancements in technology at every level of patient care, from pre-primary cate in the form of wearables, to advancements in testing and result analysis at secondary care via new robotics and AI models. This will culminate in feeding back larger amounts of accurate data to help track trends, with the aim of transitioning form a reactive healthcare model to a preventative one. It is critical though that information on innovative technology and methodologies is dissipated to healthcare professionals throughout all care levels. This will ensure that all tiers of the healthcare system are aware of what solutions exist and how they will benefit their workflows.
Some schemes have already been put into place to help lessen the burden of infections on primary care. One example in the Pharmacy First scheme, part of which allows women aged between 16 and 64 to access antibiotics for uncomplicated UTIs over the counter, following consultation with a participating pharmacist from the process with no requirement for a sample to be provided. While there are assurances that antibiotics would only be prescribed when 'clinically appropriate', 11 it is difficult to see how removing clinical diagnosis will aid antibiotic stewardship. Unsuccessful treatment plans have already been noted following this scheme, with patients presenting to primary care again following unsuccessful treatment.
The availability of innovative, high-throughput diagnostic equipment will likely be the most appropriate strategy for the improvement of diagnosis and treatment of UTIs. Providing targeted treatment more rapidly is the key. This will reduce the chance of the development of a severe infection, resulting in a decrease in emergency admissions and curbing the misuse of a broad-spectrum antibiotics. This should also to flatten the curve of AMR, adhering to last year's release of the UK Government's new 5-year AMR action plan,12 where the reduction in unnecessary prescribing and overprescribing of broad-spectrum antimicrobials in a key target.
Introducing the Mast Uri Connect
The MAST URI® Connect, an innovation of the popular Mast Uri System, aims to help clinical diagnostic laboratories recue the pressure of UTI analysis. The high-throughput system provides direct, phenotypic urinalysis, decreasing turnaround time and ensuring full sample traceability. One of the new features on the system is the implementation of expert reading rules, that are aligned ot current EUCAST breakpoint guidelines. 13 This aims to help guide the user to a clinically relevant result, by flagging non-relevant sensitivities with the goal of championing antibiotic stewardship.
One of the main benefits of the system is the fact the testing is completed directly from the urine sample, providing culture and sensitivities simultaneously. This removes the requirement for an initial culture that is routinely required for other secondary care methodologies, resulting in a 24-hour reduction in turnaround time. This will directly aid primary care, where results can currently take anywhere from three to five days to land back at a GP's desk.
One area that we are continuing to develop with the MAST URI® is our AMR portfolio. We are currently working on reformulations of our current AMR screening offerings, including updating our carbapenem-resistant Enterobacteriaceae (CRE) product to focus on carbapenemase-producing Enterobacteriaceae (CPE) instead. A poster detailing its development can be found on the Mast Group website. 14 This is as well as looking to expnad the range, to allow for the identification of more common AMR mechanisms. Much like with our alignment to EUCAST expert reading rules, we focus on antibiotic stewardship, in the shared goal of combatting AMR.
Conclusions
The burden of UTIs is felt at every level of care in the UK, from the immense number of cases to the increasing resistance to treatment. Advancements in technologies with an emphasis on proper antimicrobial stewardship are the key areas to be focused on to help relieve healthcare burden and improve patient outcomes. Government-led initiatives paint a bright future for the advancement of the healthcare system, and through the collaboration of healthcare professionals, government bodies and medical diagnostics developers, the burden of UTIs will almost certainly be reduced.
This article has been written in partnership with the general practitioners of Castlefields Health Centre, a primary care community health centre providing a vital service to over 15,000 patients in its local area of Runcorn, Cheshire. I want to thank the team for their comments, which have been indispensable in gaining a better understanding of the challenges they face with UTIs and antibiotic stewardship.
References
- 1Clinical Knowledge Summary. Urinary tract infection (lower) - men: How common is it?
(National Institute for Health and Care Excellence (NICE), 2025)
- 2Öztürk R, Murt A. Epidemiology of urological infections: a global burden
World J Urol. 2020;38(11):2669–2679. doi:10.1007/s00345-019-03071-4
- 3Martin S. What’s new in antimicrobial stewardship?
(UK Clinical Pharmacy Association, 2023) https://ukclinicalpharmacy.org/clinical/infection/whats-new-in-antimicrobial-stewardship/
- 4Palin V, Mölter A, Belmonte M, Ashcroft DM, White A, Welfare W, van Staa T. Antibiotic prescribing for common infections in UK general practice: variability and drivers
Journal of Antimicrobial Chemotherapy. 2019;74(8):2440-2450. doi.org:10.1093/jac/dkz163
- 5Tomlinson E, Ward M, Cooper C, James R, Stokes C, Begum S, Watson J, Hay A D, Jones H E, Thom H, Whiting P. Point-of-care tests for urinary tract infections to reduce antimicrobial resistance: a systematic review and conceptual economic model.
National Institute for Health and Care Research (NIHR). 2024; 28(77). doi.org/10.3310/PTMV8524
- 6UK Government. Antibiotic resistant infections continue to rise. (Gov.co.uk, 2023)
- 7UK Government. UKHSA publishes latest survey on healthcare-associated infections (UKHSA, 2025)
- 8NHS. New awareness campaign to help reduce hospital admissions for urinary tract infections. (NHS England, 2023)
- 9Sturgess I, Weinbren M, Clarke K. Automated urinalysis: a role in managing sepsis
Pathology in Practice. 2014.
- 10UK Government and NHS. Fit for the Future: 10 Year Health Plan for England Executive Summary.
- 11UK Government. Pharmacy First: what you need to know (Gov.co.uk, 2024)
- 12UK Government. Confronting antimicrobial resistance 2024 to 2029 (Gov.co.uk, 2024)